
What is Wrong?
Shoulder pain can come from a variety of pathologies. Some of the most common are:
- Shoulder Impingement / Subacromial Pain
- Rotator Cuff Tendinopathy / Tendinitis
- Rotator Cuff Tear
- Shoulder Instability
- Frozen Shoulder / Adhesive Capsulitis
Shoulder Impingement / Subacromial Pain
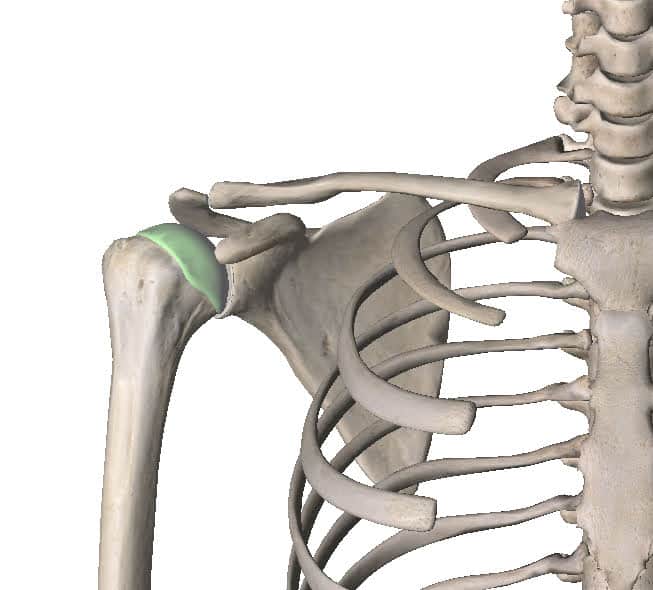
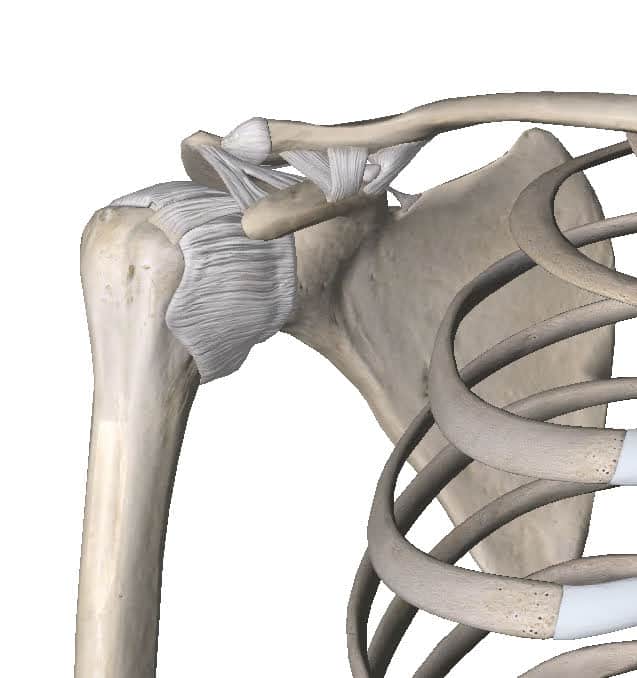
The shoulder joint is a ball and socket joint. The ball is the top of the humerus (arm) bone that sits in a little socket on the scapula (shoulder blade). That little socket is called the glenoid and so the medical name for the shoulder joint is the glenohumeral joint. The humeral head (ball) sits in the glenoid (socket) below a part of the shoulder blade called the acromion. There is a little gap between the humeral head and the acromion that we call the subacromial space. In that little space sit some fluid filled sacks known as bursae and some tendons from the shoulder muscles.
Shoulder Impingement is a term often used to refer to pain coming from that subacromial space. The tendons and bursae in that area can become irritated and painful. This will produce pain around the side of the shoulder and top of the arm. It is debatable whether this is actually an impingement problem. That’s because those structures get pinched every time anyone lifts their arm up. This is normal and it doesn’t hurt. If one of those structures is sensitive though, it does hurt.
So it may be that the impingement isn’t the problem (although experts disagree about this). A more useful term might be subacromial pain as it just states where the pain is coming from. Subacromial pain means that you have pain coming from one of the bursae or tendons in that subacromial space.
Subacromial pain affects people of all ages. It usually feels like a dull pain in the shoulder/upper arm that becomes a sharper pain as you lift the arm overhead.
Rotator Cuff Tendinopathy / Tendinitis
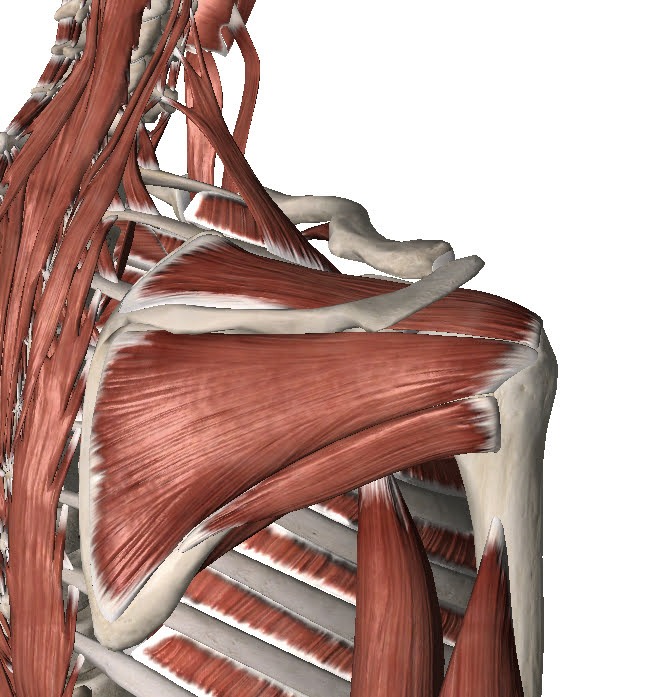
To call the shoulder joint a ball and socket joint is pretty generous really. It’s much more like a golf ball on a tee than a ball in a socket. In order to keep that ball in the socket we need the rotator cuff muscles. These are a group of 4 muscles coming from the shoulder blade and attaching to the humeral head. They work together to“suck” the ball into the socket and keep it in there as we move the arm around.
When we make any arm movement at all, the cuff is activated to suck the ball into the socket. This means it has to work very hard. As the saying goes…
“It’s tough being a cuff”
All muscles become tendons before they attach to a bone. While the muscle is the red part that contracts, the tendon is the white part that doesn’t contract, it just transmits the force of the muscle into moving the bone. The rotator cuff muscles are no different.
Sometimes those tendons become painful and sensitive. We call this tendinopathy. An older term for the same problem was tendinitis. Most health professionals stopped using that term a while ago as it’s not technically accurate, but it’s not such a big deal so some people still use it. Tendinopathy is a fusion of the words tendon and pathology (which literally means tendon-problem).
Rotator cuff tendinopathy is when the shoulder pain is coming specifically from changes in the tendon. These changes are thought to be related to long term overloading of the tendon. Essentially, tendons hurt when they’re not strong enough to do their job. The tendon becomes sensitive and painful when loaded.
Rotator cuff tendinopathy affects people of all ages but is rare in youngsters. It feels similar to subacromial pain in that you feel a dull pain in the shoulder and upper arm that becomes sharper and more intense when the arm is raised overhead.
Rotator Cuff Tear
You can develop tears in the rotator cuff muscles or tendons. This can be from a single incident or they can develop gradually. When they develop gradually they often come on in association with rotator cuff tendinopathy. The tears can span from a tiny little slit to a complete severance of the muscle/tendon. This means that the problem can range from very minor to very severe.
Interestingly, small tears in the rotator cuff seem to be a normal part of aging that doesn’t cause any problems. In fact, the majority of elderly people will have some tears in their cuff that cause no symptoms. However, sometimes even a small tear can cause quite a bit of pain and limit your ability to use your arm. A massive tear will result in significant weakness. Many people with a massive cuff tear can’t even lift their arm overhead.
With such a wide spectrum of injury, it can be difficult to determine if a rotator cuff tear is what is causing the problem. Imaging such as ultrasound scans and MRI scans can be helpful here.
Pain from a rotator cuff tear is usually felt in the shoulder and upper arm as a dull ache. When lifting the arm the pain becomes sharper. If the tear is large you may have trouble actually getting the arm to lift overhead. These injuries are more common in the middle aged and older population, particularly in sporty people.
Shoulder Instability
The shoulder is a ball and socket joint between the humeral head and glenoid. The ball is the top of the humerus (arm) bone that sits in a little socket on the scapula (shoulder blade). That little socket is called the glenoid.
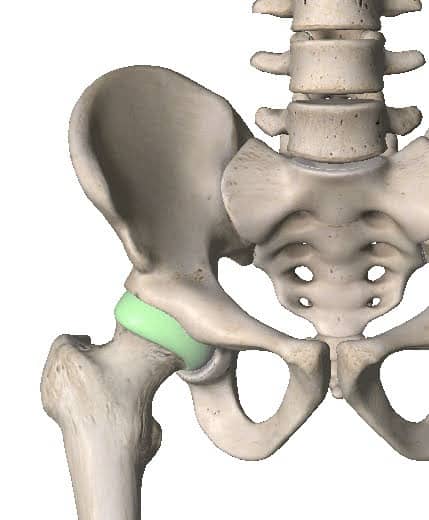
The design of the shoulder is inherently unstable. Nature has it this way because we like to have lots of movement available at the shoulder. In this way we have sacrificed stability in favour of mobility. Both the hip and the shoulder are ball and socket joints. However, the hip is very stable where the shoulder is quite unstable.
This is a good thing as we like having lots of mobility in our shoulder. It lets us lift our arms overhead and reach back behind us. It gives our incredibly dexterous hands a wide field of influence! However, the cost of freedom is eternal vigilance. Our rotator cuff muscles have to work extremely hard to keep that ball in the socket. They have a little help from some other connective tissues like the labrum and the glenohumeral ligaments.
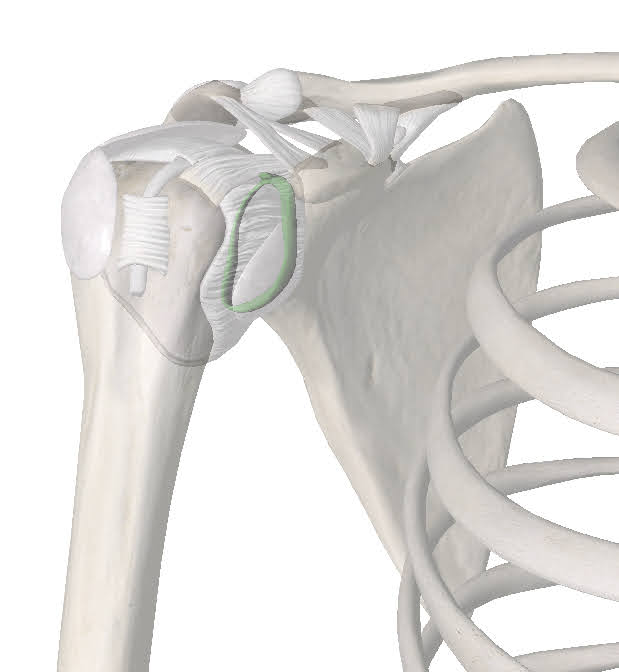
Sometimes though, the system fails. If the cuff muscles and the connective tissues can’t keep the ball in the socket it will roll out, usually forwards. We call that a dislocation. When that happens sometimes you can shove it back in, but usually you will need a doctor to do it for you. When the dislocation occurs it can damage some of those connective tissues like the labrum and glenohumeral ligaments. If this happens the shoulder can be prone to rolling out in the future, we call that shoulder instability. Sometimes the shoulder doesn’t roll out of the socket completely. It just moves out of place a bit. We call this a subluxation rather than a dislocation.
Shoulder instability is more common in younger people. Particularly in young girls who are very flexible. It can also become a problem after a large trauma to the shoulder, in a tackle during a football game for example. THe shoulder often feels “loose” and will sometimes “clunk”. People often describe it “feeling unstable”. When the shoulder subluxes or dislocates it is usually accompanied by severe pain, but sometimes is oddly painless.
Frozen Shoulder / Adhesive Capsulitis
Surrounding the ball and socket of the shoulder joint we also have a fibrous joint capsule. This capsule is made of collagen which is a bit stretchy. This stretchiness allows the shoulder to move.
Unfortunately, sometimes that joint capsule becomes very stiff. The collagen loses its stretchiness and the inner lining of the capsule becomes inflamed and painful. We call this condition Adhesive Capsulitis but it is more commonly known as frozen shoulder.

We don’t know why this happens. Adhesive capsulitis is an auto-immune disorder, meaning that the body’s immune system is attacking itself. Frozen shoulder usually lasts a long time, 1 to 2 years (perhaps even longer).
It is characterized by different stages. Sometimes these stages are referred to as freezing, frozen and thawing. The freezing stage is usually intensely painful. Often giving significant pain at rest and disturbing sleep. The frozen stage is less painful but the shoulder remains incredibly stiff and it is impossible to lift the arm overhead or reach up behind your back. The thawing stage is when the shoulder starts to loosen up again.
Frozen shoulder usually affects middle aged people. It’s far more common in women and diabetics. Unfortunately, those who get one frozen shoulder have a high chance of getting another on the other side.
How Long Will My Shoulder Pain Last?
That really depends on what the pathology is. Subacromial pain and rotator cuff tendinopathy would be expected to resolve within 3 months with proper rehabilitation. A rotator cuff tear may require surgery as might shoulder instability. Frozen shoulder can be expected to last at least 1-2 years.
Do I need an x-ray or MRI?
Again, this depends on what pathology is causing your shoulder pain. Often these conditions can be diagnosed through a clinical examination by a doctor, physiotherapist, chiropractor or athletic therapist. A clinical examination involves physical tests and questions to determine the nature of the problem. This helps narrow the cause down to one of 2-3 potential causes or can even narrow it down to just one clinical diagnosis.
If it is not 100% clear what the pathology is after the clinical examination then you may be referred for imaging. Imaging includes things like x-rays, MRIs, CT or ultrasound scans. These images help the clinician determine what the pathology is.
If an appropriate treatment plan can be made from the clinical examination then there is no need to get imaging studies done. This is usually the case. Since most problems will respond well to conservative management the first port of call is usually rehabilitation. If you are not improving within a reasonable period of time then it may be worth reviewing the clinical diagnosis and the treatment plan. At that point your clinician may refer you for imaging.
It is important to note that clinicians should only refer people for imaging if the results of the imaging would change the treatment plan. For example, your clinician may perform a clinical examination and then say:
“Well, it’s either subacromial pain or rotator cuff tendinopathy. Either way I’d recommend 6 weeks of Athletic Therapy”
In this case imaging would not be helpful as the treatment plan would be the same regardless of the results. However, after the clinical exam your clinician could say:
“It looks like rotator cuff tendinopathy but I’m a bit worried it might be frozen shoulder. If it’s frozen shoulder I’m going to refer you to a specialist to consider a corticosteroid injection. If it’s rotator cuff tendinopathy you can go for Physio. So we’ll order an ultrasound scan to see which it is”
In this situation, the results of the imaging would influence the treatment plan. So it is appropriate to order the scan.
What should I do?
There are lots of things you can do to make this less unpleasant and speed up the resolution of your pain. What you ultimately decide to do will depend on your circumstances.
Consult a Professional
This would certainly be my top pick. While the other things on this list will definitely be helpful, there really is no substitute for the guidance and expertise of a professional. It’s like doing your tax return, you can certainly do it yourself, but it would be much easier and more effective to consult an accountant. So the first question is which type of professional? This is where I’m going to show my own bias a little. As a physiotherapist, I honestly feel like a rehabilitation professional such as a Physio, Athletic Therapist or Chiropractor would be the best person to see first.
These professionals can do a full assessment and provide a clinical diagnosis. They can refer you to the appropriate doctors or surgeons for scans and further testing if they feel it is needed. They can also help you understand the problem and design a rehabilitation program that will help you recover as fast as possible.
We have all of these professionals available here at Collegiate Sports Medicine. If you would like to have a chat with us about how we might be able to help, we’d love to hear from you. Just give us a call.
Symptom Guided Activity
This may sound like a strange term. The idea is to stay active but only to the degree that you feel able. I like to use a green light, orange light and red light system. Green is no pain, orange is mild pain and red is severe pain. Generally speaking, you can do whatever you want as long as you feel no pain or mild pain. If the pain becomes severe, you have to stop. Over time, you will find you are able to be more and more active.
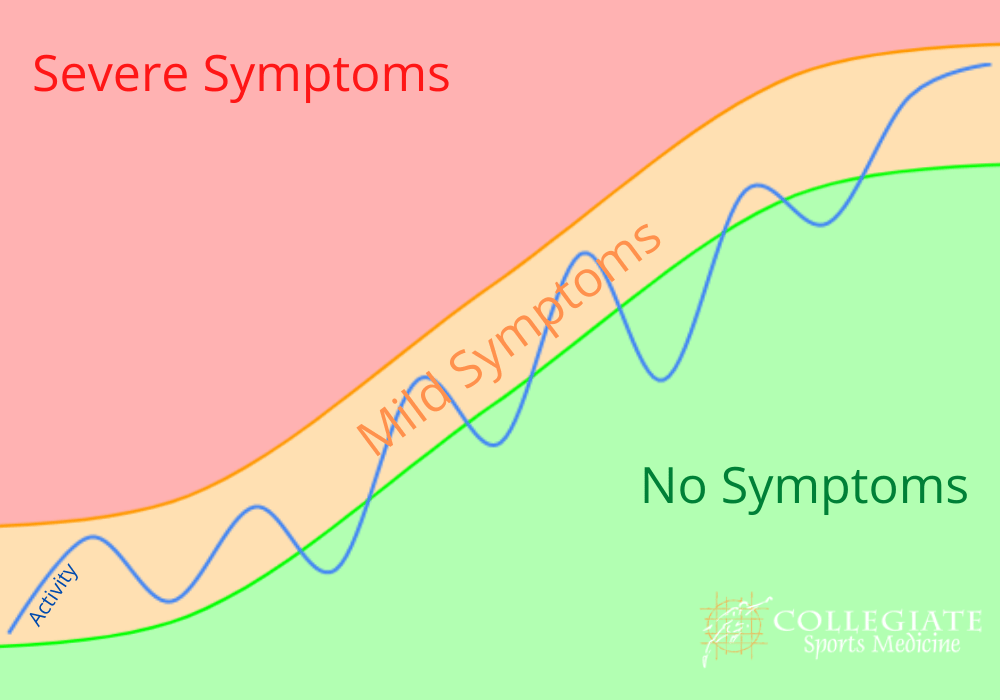
In this sense, no activity is “off limits.” You can go to work, play sports, go for a run, lift weights, go swimming, go camping … whatever you like. Your only restriction is that you must try to avoid that severe “red light” pain. If doing any of these causes severe pain, then leave it till next week and try again!
Manual Therapy
Manual Therapy includes treatments like soft tissue massage and joint mobilisations. There are many different kinds of therapy and different therapists who will have different skills. This is certainly something you may discuss with your therapist should you decide to work with a professional. There are a few things you can do at home such as using a tennis or lacrosse ball to help loosen up the muscles. Again, the traffic light rules apply. There should be no severe “red light” pain. If there is, you need to go more gently.
Just press the ball up against the back of your shoulder between you and a wall or the floor. Move around to work the ball as if the ball is giving you a massage. You can do this for as long as you like but I would suggest starting with about 3 minutes and then see how you feel afterwards.
Summary
Shoulder pain can be coming from a variety of different causes or pathologies. It is not really possible to diagnose it accurately on your own. You would need the input of a doctor, physiotherapist, chiropractor or athletic therapist. The best way to manage the problem really depends on what the diagnosis is. If you would like some advice just give us a call.
Matthew Boyd, Physiotherapist