What is causing my knee pain?
Knee pain can come from a variety of pathologies. Some of the most common are:
- Knee Arthritis / Osteoarthritis
- Patellofemoral Pain
- Meniscal Tear
- Patellar Tendonitis / Tendinopathy
- IT Band Syndrome
- Ligament Tear
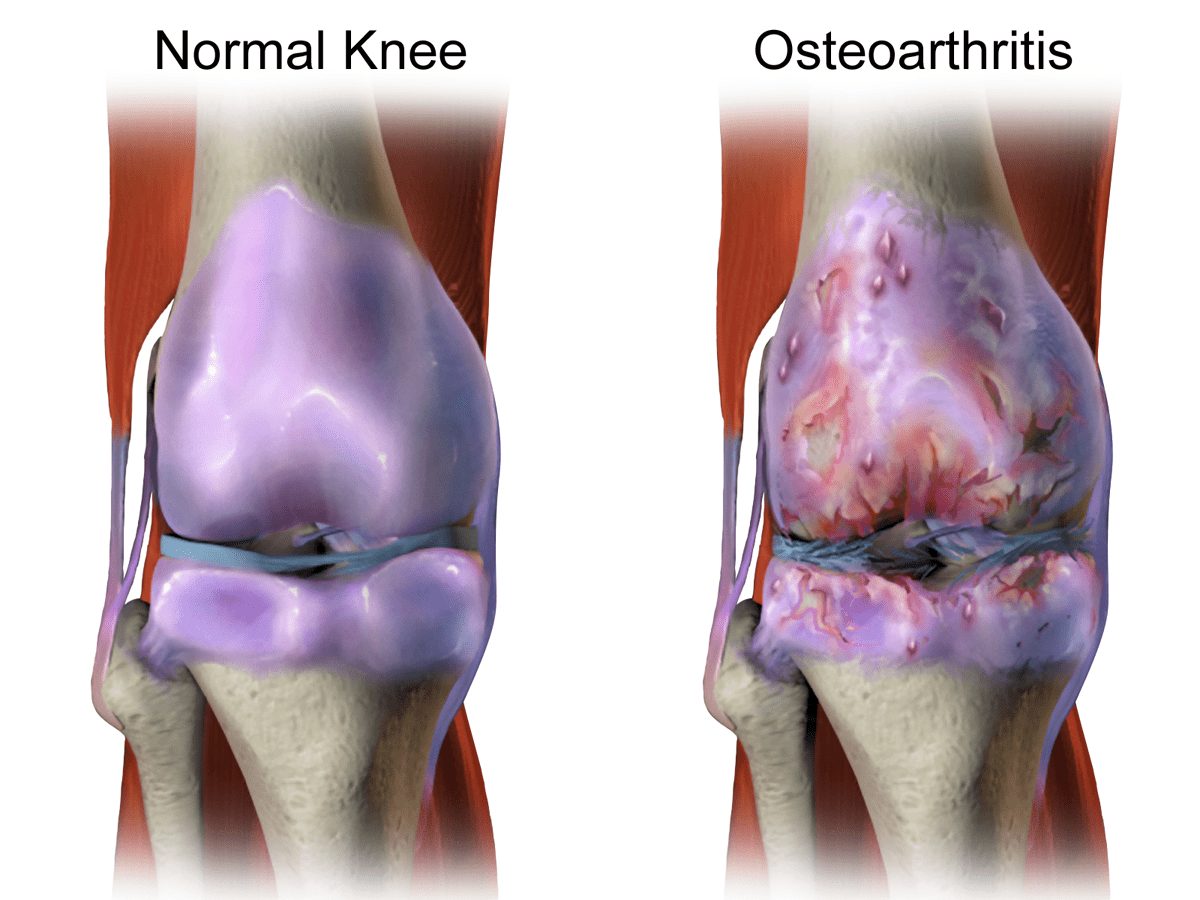
Knee Arthritis / Osteoarthritis
The knee is a hinge joint between the femur (thigh bone) and the tibia (shin bone). The ends of the bone (joint surfaces) are lined with hyaline cartilage and a shock absorbing tissue called the meniscus sits between the two bones.

Arthritis is a term used to describe the general deterioration of the joint surfaces over time. That hyaline cartilage can break down and this can allow irritation of the underlying bone. We call this Osteoarthritis but it is often abbreviated to arthritis.
Osteoarthritis is actually a normal part of ageing. All joints will degenerate over our lifetime. Just as we develop wrinkles in our skin, we develop arthritis in our joints. Most of the time this arthritis doesn’t hurt. This has led some medical professionals to differentiate between symptomatic and asymptomatic osteoarthritis. The problem usually arises when the joints are degenerating quicker than we would expect. If a 40 year old man has the level of arthritis that we would expect in an 80 year old, that’s a problem and it may be causing knee pain. However, if the amount of arthritis the 40 year old man has is what we would expect in a 40 year old man, that’s fine.
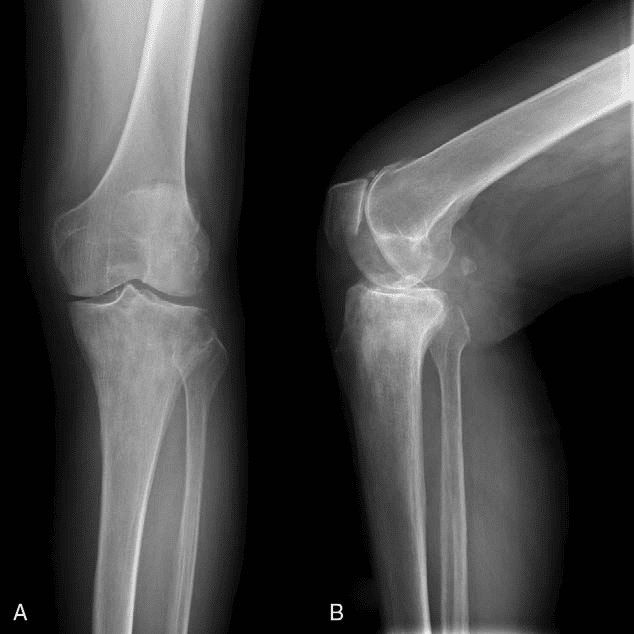
The other tricky bit is that it doesn’t always hurt. Sometimes you can have significant osteoarthritic change in a joint that is completely pain free. This makes for a very confusing picture. If someone has arthritic change on their x-ray, then we need to compare that to their symptoms in order to decide if it’s a problem or not.
Symptomatic Knee Osteoarthritis is more common in the older population but can sometimes be an issue in the middle-aged. It is more common in women. It usually manifests as a general aching pain in the knee that will be worse with weight bearing activities like walking, running or just being on your feet for a long time.
Patellofemoral Pain
The patella (kneecap) is a sesamoid bone within the quadriceps (thigh) muscle tendon. A sesamoid bone is basically a small piece of bone living within a tendon. A tendon is the strong connective tissue that attaches our muscles to our bones. Muscles become tendons before they attach to bones.
We have a patella because as the knee bends the quadriceps tendon is bent around the femur (thigh bone) and this squashes the tendon up to the bone. If we didn’t have a patella the tendon would fray and break. Nature gives us this natural barrier in the form of the patella to prevent the tendon from being damaged.
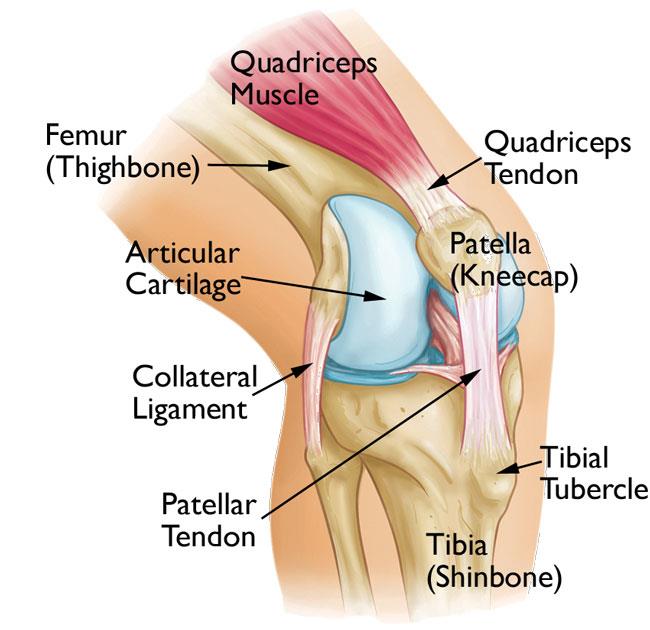
In this way the patella protects the quadriceps tendon by pressing up against the femur when the knee bends (so the tendon doesn’t have to). The back of the patella has an articular surface that pushes up against a similar articular surface on the femur. We call the articulation (interaction) between the patella and the femur the patellofemoral joint. When you bend your knees while standing, walking or running you cause the patella to push up against the femur. We call this loading the patellofemoral joint.
When that articular surface on the back of the kneecap (patella) becomes irritated and painful we call it patellofemoral pain.
Patellofemoral pain is more common in younger people. Especially among young athletes or people getting into new sports like running. It’s very common in runners and for this reason it is sometimes referred to as runner’s knee. The pain usually feels like it is actually behind the kneecap. However, it can also be felt as a diffuse pain within the knee or even at the back of the knee!
Meniscal Tear
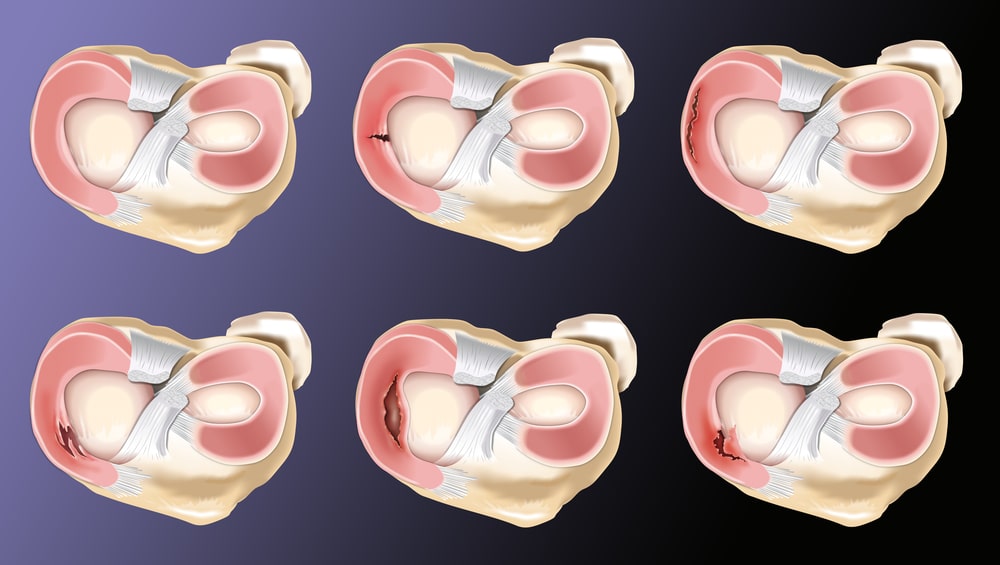
Between the femur (thigh bone) and the tibia (shin bone) we have a shock absorbing tissue called the meniscus. There is actually one on the inner side of the knee and one on the outer side. So we have two menisci (plural) in each knee. The primary role of the menisci is to be a shock absorber between the two major bones of the leg. So it’s pretty tough being a meniscus!
It’s easy to develop fraying or tearing of the meniscus as we age. We call these little “wear and tear” signs “degenerative tears” of the meniscus. We can also have a sudden traumatic tear of one of the menisci (during a sporting injury for example). Depending on the type of tear and how it was sustained, it will look a little different:
Meniscal tears are rare among young children. Sporty adolescents and younger adults sometimes sustain traumatic tears to the meniscus. Degenerative tears (fraying) are much more common among middle aged people. Traumatic tears can sometimes cause “locking” of the knee – meaning it gets stuck and wont move. The degenerative tears can cause more aching type of pain which will be worse with activity.
Patellar Tendinopathy
Tendons are the stiff, fibrous parts of muscles that attach to bones. The quadriceps muscle of the thigh has a quadriceps tendon to attach it to the tibia (shin bone). Inside the quadriceps tendon we have the patella (kneecap). So the quadriceps tendon actually becomes the patella tendon before attaching to the tibia (shin).

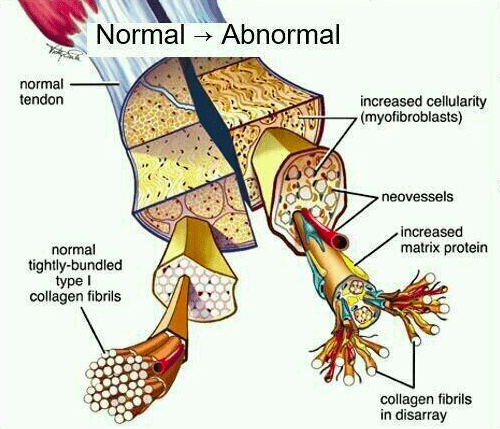
When that patella tendon becomes painful it is called patella tendonitis. Technically speaking patella tendinopathy is a more accurate term, but both are used regularly. Tendinopathy refers to changes in the cellular structure of the tendon. The collagen bundles that make up the tendon become disorganized and sensitive.
Patellar Tendinopathy is common in younger athletes. Especially teenagers who play jumping sports like volleyball or basketball. For this reason it is sometimes referred to as “jumper’s knee”. It feels like a very specific pain in a small area just below the kneecap. It is usually completely pain free at rest but provoked by activity. It will definitely be worse during or after sports involving sprinting or jumping.
IT Band Syndrome
The IT Band is a large band of connective tissue coming from the Gluteus Maximus and Tensor Fascia Latae muscles of the hip. The two muscles join together on the side of the leg and form the Iliotibial Band or IT Band. The IT Band is a large flat tract of connective tissue made of strong, ropey like fibres of collagen. It comes down the side of the thigh and attaches into the side of the tibia (shin bone). Being a very strong connective tissue at the side of the knee allows the IT Band to offer some lateral (side) stability to the knee joint.
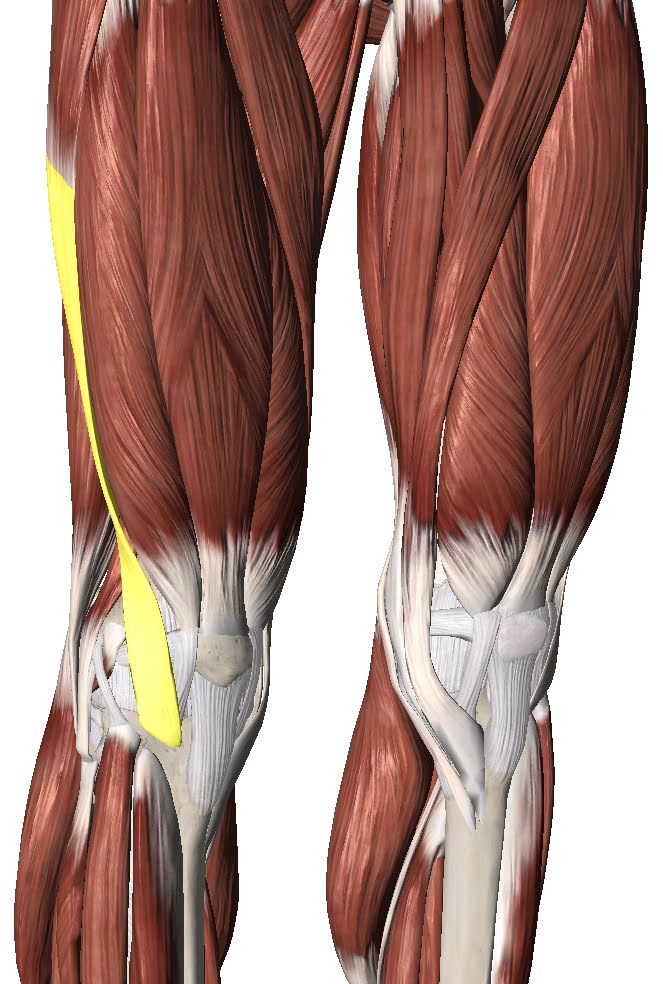
The IT Band can become irritated and painful at the point where it inserts into the tibia just at the side of the knee. We call this IT Band Syndrome.
IT Band Syndrome usually affects people who do very repetitive activities like running, cycling or hiking. It is often worse going downhill with running or cycling but not always. It feels like a sharp pain right on the outside of the knee. It will usually get gradually worse as you continue the run/ride/hike until it becomes very painful.
Ligament Tear
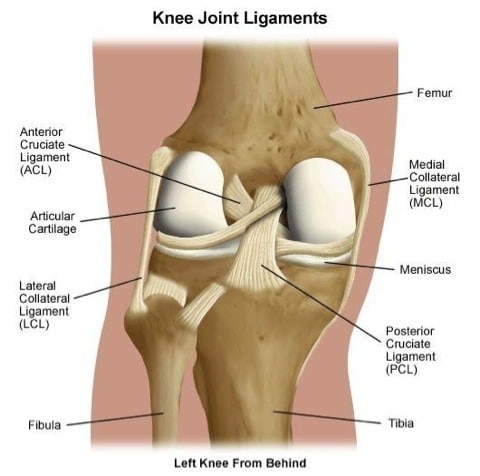
Ligaments are little strips of connective tissue that we have around our joints to give them stability. The knee has many ligaments, the most important are the medial and lateral collateral ligaments and the anterior and posterior cruciate ligaments.
Tears to these ligaments are always the result of trauma. When we tear a ligament fully or partially we call it a sprain. Depending on how much of the ligament is torn, the sprain would be classified as grade 1, 2 or 3. Medial collateral ligament sprains are fairly common. Lateral collateral ligament sprains are extremely rare. Cruciate ligament sprains happen often in younger people who play sports. An Anterior Cruciate Ligament sprain is a very serious injury and often requires surgery.
The sprain is usually experienced as pain and swelling after a traumatic injury – such as twisting the knee too much while playing sport. If the sprain is bad enough you may also experience instability or “giving way” of the knee which means it “buckles” underneath you.
How Long Will My Knee Pain Last?
That really depends on what the pathology is. Knee Osteoarthritis can last many years and may get progressively worse. Patellofemoral pain or IT band syndrome may go away if you reduce your activity levels but it will come back when you return to the activity. Meniscus tears and ligament sprains can often be rehabilitated within 6-12 weeks but may require surgery (depending on the severity).
Do I need an x-ray or MRI?
Again, this depends on what pathology is causing your knee pain. Often these conditions can be diagnosed through a clinical examination by a doctor, physiotherapist, chiropractor or athletic therapist. A clinical examination involves physical tests and questions to determine the nature of the problem. This helps narrow the cause down to one of 2-3 potential causes or can even narrow it down to just one clinical diagnosis.
If it is not 100% clear what the pathology is after the clinical examination then you may be referred for imaging. Imaging includes things like x-rays, MRIs, CT or ultrasound scans. These images help the clinician determine what the pathology is.
If an appropriate treatment plan can be made from the clinical examination then there is no need to get imaging studies done. This is usually the case. Since most problems will respond well to conservative management the first port of call is usually rehabilitation. If you are not improving within a reasonable period of time then it may be worth reviewing the clinical diagnosis and the treatment plan. At that point your clinician may refer you for imaging.
It is important to note that clinicians should only refer people for imaging if the results of the imaging would change the treatment plan. For example, your clinician may perform a clinical examination and then say:
“Well, it’s either patellofemoral pain or patellar tendinopathy. Either way I’d recommend 6 weeks of Athletic Therapy”
In this case imaging would not be helpful as the treatment plan would be the same regardless of the results. However, after the clinical exam your clinician could say:
“It looks like patellofemoral pain but I’m a bit worried it might be osteoarthritis. If it’s osteoarthritis I’m going to refer you to a specialist. If it’s patellofemoral pain you can go for Physio. So we’ll order an x-ray to see which it is”
In this situation, the results of the imaging would influence the treatment plan. So it is appropriate to order the scan.
What should I do?
There are lots of things you can do to make this less unpleasant and speed up the resolution of your pain. What you ultimately decide to do will depend on your circumstances.
Consult a Professional
This would certainly be my top pick. While the other things on this list will definitely be helpful, there really is no substitute for the guidance and expertise of a professional. It’s like doing your tax return, you can certainly do it yourself, but it would be much easier and more effective to consult an accountant. So the first question is which type of professional? This is where I’m going to show my own bias a little. As a physiotherapist, I honestly feel like a rehabilitation professional such as a Physio, Athletic Therapist or Chiropractor would be the best person to see first.
These professionals can do a full assessment and provide a clinical diagnosis. They can refer you to the appropriate doctors or surgeons for scans and further testing if they feel it is needed. They can also help you understand the problem and design a rehabilitation program that will help you recover as fast as possible.
We have all of these professionals available here at Collegiate Sports Medicine. If you would like to have a chat with us about how we might be able to help, we’d love to hear from you. Just give us a call.
Symptom Guided Activity
This may sound like a strange term. The idea is to stay active but only to the degree that you feel able. I like to use a green light, orange light and red light system. Green is no pain, orange is mild pain and red is severe pain. Generally speaking, you can do whatever you want as long as you feel no pain or mild pain. If the pain becomes severe, you have to stop. Over time, you will find you are able to be more and more active.
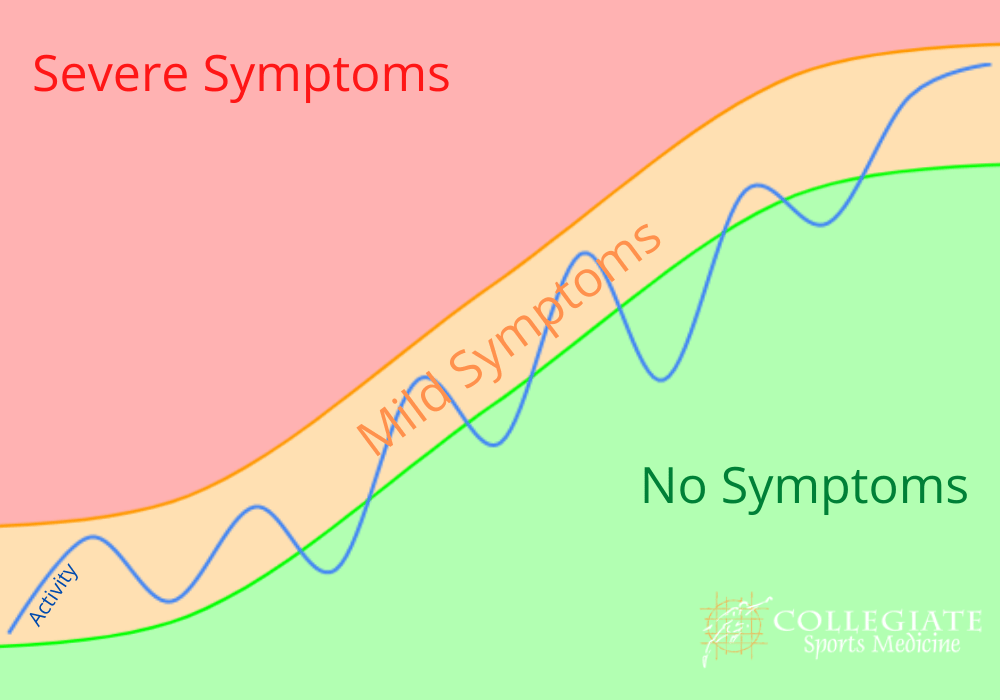
In this sense, no activity is “off limits.” You can go to work, play sports, go for a run, lift weights, go swimming, go camping … whatever you like. Your only restriction is that you must try to avoid that severe “red light” pain. If doing any of these causes severe pain, then leave it till next week and try again!
Summary
Knee pain can be coming from a variety of different causes or pathologies. It is not really possible to diagnose it accurately on your own. You would need the input of a doctor, physiotherapist, chiropractor or athletic therapist. The best way to manage the problem really depends on what the diagnosis is. If you would like some advice just give us a call.